![]()
‘I Don’t Believe in God, but I Believe in Lithium’
My 20-year struggle with bipolar disorder.
The manila folder is full of faded faxes. The top sheet contains a brief description of my first medically confirmed manic episode, more than 20 years ago, when I was admitted as a teenager to U.C.L.A.’s Neuropsychiatric Institute: “Increased psychomotor rate, decreased need for sleep (about two to three hours a night), racing thoughts and paranoid ideation regarding her parents following her and watching her, as well as taping the phone calls that she was making.”
I believed I had special powers, the report noted; I knew ‘‘when the end of the world was coming due to toxic substances’’ and felt that I was the only one who could stop it. There was also an account of my elaborate academic sponsorship plan so I could afford to attend Yale — some corporation would pay for a year of education in exchange for labor or repayment down the line. (Another grand delusion. I was a B-plus student, at best.)
After I was admitted to the institute’s adolescent ward, I thought the nurses and doctors and therapists were trying to poison me. So was the TV in the rec room. I warned my one friend in the ward that its rays were trying to kill him. The generator outside my window was pumping in gas. The place, I was sure, was a death camp.
I refused meds because they were obviously agents of annihilation. It took four orderlies to medicate me: They pinned me to the floor while a nurse plunged a syringe into my left hip. Over time, I became too tired to refuse medication. Or perhaps the cocktail of antipsychotics started working. The Dixie cup full of pills included lithium, which slowly took hold of my mania. After a few weeks, I stopped whispering to the other patients that we were all about to be killed. Eventually, I stopped believing it myself.
Mark DeAntonio, the U.C.L.A. psychiatrist who was treating me, said I had bipolar disorder. Here’s the phrasing from the National Institute of Mental Health: ‘‘unusually intense emotional states that occur in distinct periods called ‘mood episodes.’ Each mood episode represents a drastic change from a person’s usual mood and behavior. An overly joyful or overexcited state is called a manic episode, and an extremely sad or hopeless state is called a depressive episode.’’ The generic definition doesn’t quite cover the extremes of the disease or its symptoms, which include inflated self-esteem, sleeplessness, loquaciousness, racing thoughts and doing things that, according to the Mayo Clinic, ‘‘have a high potential for painful consequences — for example, unrestrained buying sprees, sexual indiscretions or foolish business investments.’’
I was only 17, young at that time to receive a bipolar diagnosis. Most of the teenagers on the ward were there for eating disorders or depression. I had to eat my meals alone because my food intake wasn’t restricted or monitored, as it was for everyone else. I made moccasins in occupational therapy and played volleyball with the eating-disorder girls in recreational therapy. I went from being locked in solitary confinement, clawing at the soft brown walls, to being granted TV privileges. I was even allowed to hold the remote and choose the channel. Visitors came and left presents and balloons and a big get-well note on poster board signed in puffy paint and Sharpies by all my high-school friends.
Lithium, a mood stabilizer that can help stop and prevent manic cycles, is usually the first medication tried with bipolar patients; it’s effective for most of them. Including me. I was discharged and sent back to high school with an apple-size bruise on my hip. For two decades since then, I have been taking lithium almost continuously. It has curbed my mania, my depression and, most significant, the wild delusional cycles that have taken me from obsessing over the value of zero to creating a hippie cult (my uniform: bell-bottoms, psychedelic sports bra and body glitter, head to toe). As long as I take those three pink lithium-carbonate capsules every day, I can function. If I don’t, I will be riding on top of subway cars measuring speed and looking for light in elevated realms.
The use of lithium as a therapy for mental illness goes back to at least Greek and Roman times, when people soaked in alkali-rich mineral springs to soothe both ‘‘melancholia’’ and ‘‘mania.’’ In the mid-1800s, lithium was thought to cure gout and sometimes ‘‘brain gout,’’ a lovely description for mania, extending the notion of swollen joints to a swollen brain. The element gets its name from lithos, the Greek word for stone, and lithium is indeed found in granite — and in seawater, mineral springs, meteorites, the sun and every other star and all humans. It is classified as a metal on the periodic table of elements. It was first identified as a solid in the form of petalite ore on the Swedish island Utö in 1817. A year later, scientists found that lithium, when ground into powder, turned flames crimson red — it’s the key ingredient in red fireworks. Fiery and unstable, lithium somehow calms emotional states often characterized in the same way.
Despite the fact that people have benefited from its use for millenniums, how lithium works upon brains is largely unknown. ‘‘It has so-called trophic or fertilizing activity on the brain — that is, it stabilizes membranes,’’ says James Kocsis, a professor of psychiatry at Weill Cornell Medical College in New York and an expert on lithium. But the actual mechanics are a mystery. One way to think about its effect, though, is suggested by a 2007 U.C.L.A. study that found that bipolar patients taking lithium had significantly more gray matter than their counterparts, especially in the region associated with a person’s capacity to maintain attention and emotional control.
One of the first references to lithium in a neurological context appears in 1870, by a neurologist in Philadelphia named Silas Weir Mitchell, who recommended the compound lithium bromide as an anticonvulsant and a hypnotic for epileptic patients. But by the turn of the century, medical lithium had largely been supplanted by other treatments. Then, in 1947, John Cade, a psychiatrist working in a hospital outside Melbourne, Australia, rediscovered its medicinal potential. Cade was among the first to conclude that mental illness included bodily manifestations and thus should be treated with medication, not just talk therapy. ‘‘It required a change in how people understand mental illness,’’ says Robert Beech, an assistant professor of psychiatry at Yale University who conducts studies of medical lithium. He describes this insight as a shift from ‘‘more psychological, Freudian explanations to a biological explanation.’’

Cade, whose father was also a psychiatrist, was at first simply trying to isolate the cause of mania. Having noticed that the urine of manic patients was unlike that of his stable subjects, he figured the distinguishing component, uric acid, was responsible for the mania. Seeking to produce that mania in his animal subjects, guinea pigs, he needed a solution in which to supply the uric acid to them, and he chanced to use lithium urate (and later, lithium carbonate). But his guinea pigs became lethargic; instead of inducing mania, he had accidentally discovered a treatment. Cade became convinced lithium could cure many of his patients experiencing symptoms we now associate with schizophrenia, bipolar disorder, post-traumatic stress disorder and dementia. To test its safety, he ingested lithium himself; later, he began a trial with 19 patients. The 10 manic subjects experienced a significant shift in mood and function, but Cade’s timing was unfortunate. One of his subjects died, probably from a high dose. And toward the end of the ’40s, lithium’s use as a table-salt substitute for congestive heart patients in the United States proved lethal in at least two instances.
But even as these outcomes hindered the widespread application of lithium, studies continued in a number of countries. Gradually, after dosages approached uniformity and careful monitoring became routine, lithium in various compounds was recognized as an acceptable treatment. Lithium gluconate was approved in France in 1961, lithium carbonate in Britain in 1966, lithium acetate in Germany in 1967 and lithium glutamate in Italy in 1970. Among the drug’s champions was an American medical resident named Ronald Fieve, who began experimenting with lithium in 1958, after his adviser at Columbia University returned from Australia with tales of Cade’s experiment. ‘‘It was so effective,’’ Fieve told me, that he was ‘‘treating the most severe bipolar 1 patients, and this lithium brought them back to normalcy in 10 to 15 days.’’
It was not until 1970 that Fieve, now a doctor, and four other psychiatrists successfully lobbied the Food and Drug Administration to approve lithium as a psychiatric medication. ‘‘The F.D.A. was reluctant,’’ he says, ‘‘but we brought enough data that this was a new superb drug for bipolar and that if it was monitored properly, it would be safe.’’
Fieve says that lithium hasn’t been extensively tested as a treatment for other conditions in part because it’s a natural substance: Elements on the periodic table can’t be patented. Pharmaceutical companies therefore have little incentive to promote lithium or develop other uses for it, despite its potential. It has shown promise as a therapy for Alzheimer’s, for example. A study in Japan has shown a sample population to be less likely to commit suicide after drinking tap water containing lithium. In the ’30s and ’40s, 7-Up included lithium citrate as a mood-booster. There were ‘‘lithia beers’’ and a lithium version of Coca-Cola. As recently as last fall, a psychiatrist posed the question on the Op-Ed page of The New York Times: ‘‘Should we all take a bit of lithium?’’
Despite its widespread use as a mood stabilizer, only 5 percent of all lithium production is devoted to medication. The rest goes into things like ceramics, glass and batteries. The tech and electronics industries especially are becoming dependent on the element. A new highway soon to be built will connect the only American lithium mine in operation, Rockwood Lithium, in Silver Peak, Nev., to the northern part of the state, where Elon Musk is currently constructing a billion-dollar ‘‘gigafactory’’ to manufacture lithium-ion batteries for his Tesla automobiles.
Rockwood is probably where my pink pills come from. In May, I visited Silver Peak, where David Klawitter, a mechanic at the mine, showed me his swollen red hands. ‘‘The lithium burns sometimes,’’ he said. ‘‘It eats sockets, though, rusts them up solid. You can see what it does to the trucks.’’ In the mid-’60s, Rockwood’s predecessor company, Foote Mineral, located its plant in this mineral-rich wasteland after establishing a method to extract lithium from underground brine. ‘‘We make medical-grade lithium here,’’ Klawitter said. ‘‘We’re processing a pure form of lithium, the purest.’’
Along a dusty road not far from Silver Peak is Alkali Hot Spring, once the bathing grounds for tent-city miners and frontiersmen like the Earp brothers who prospected for gold at the turn of the last century. Hoses now bring lithium water, at about 100 degrees Fahrenheit, from the springs to two tubs where the locals still take the waters.
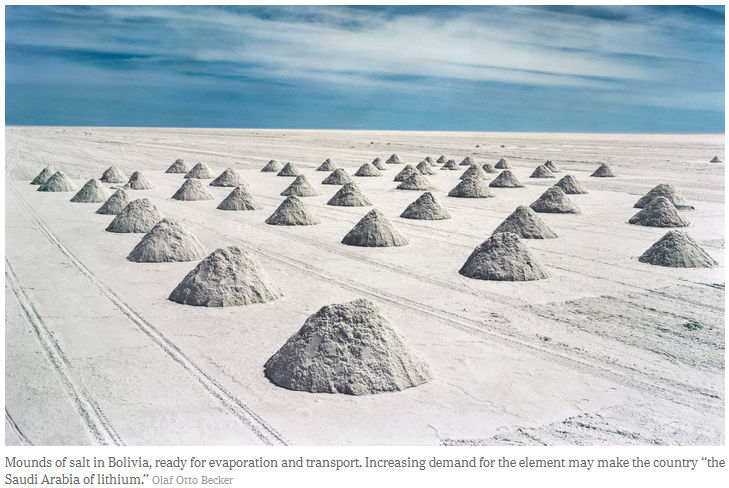
An even larger deposit of lithium, an estimated 50 percent of the world’s supply, lies beneath the Salar de Uyuni in southern Bolivia. The increasing global demand for lithium has prompted many proclamations, including claims by Bolivians that the landlocked socialist country will become the ‘‘Saudi Arabia of lithium.’’ Economists have been forecasting a lithium economy for decades, and it may well be that someday every car, computer and wearable electronic device — not to mention our energy storehouses — will depend on lithium batteries the way I’ve relied on medicinal lithium for the last 20 years.
By 2000, I had gone seven years without a manic episode. I graduated from the University of California, Davis, with degrees in English and art. I moved to New York and was leading what seemed like a regular life, writing about music for The Village Voice and painting. I went to work every day and paid my rent. If you had met me on the street, I’ll bet you would have thought: This person is normal, has normal problems, approaches the world in a normal way. I decided, along with my psychiatrist of a couple years, Henry Schwartz, to taper off the lithium. Possibly I had been given the wrong diagnosis as an adolescent. Maybe I was past the point of having manic episodes.
After a few months off lithium, I felt energetic, engaged, even electric. It’s hard to know if that feeling was just a ramping up toward mania again or if it was the lifting of a lithium fog. But this is what ended up happening: I turned down jobs and burned all professional bridges with sharp and illogical emails, many of them referring to Eminem; I kept a stash of homemade granola in my pocket to hand out to anyone who would accept a stranger’s dirty pocket granola; I developed an alter ego, a rapper named Jamya; I painted my face with spectacular green-and-gold eye shadow; I was kicked out of a bar without even drinking; I stood on my head every morning; my apartment burned down; I served as the sole witness to a stranger’s wedding on top of the World Trade Center; I wore 800 necklaces and spoke in a slow growl or sometimes a high-pitched squeal; I saved a corgi from being hit by a cab on Central Park West (on which occasion Ben Vereen stopped to call a dog ambulance); I spoke to strangers with the intensity of a car salesman stuck in a Mamet monologue; I preached about Jesus wherever I went, which for a Jew is unusual; I spent almost $700 on butternut squash and assorted seasonal gourds. My clothes smelled of fire, from the burned-out apartment. I scared the scary people on the subway. All that took place over two weeks, maybe three, as I made my way back and forth between Los Angeles and New York.
It was kumquat season and I wanted to be back in New York with Mike, a crush I met a month earlier. He worked in a start-up on the floor below my apartment. In the weeks after the fire, he followed me around with a video camera, mostly because I told him to. A few years ago, he sent me a few scenes on a VHS tape he had stashed away in his parents’ lake house. I watched it recently. I looked pretty and young and magnetic and so crazy. My face was less creased with worry and my hair was coiffed in a deep red Afro, framing perfectly shaped eyebrows. I was sporting my trademark manic style — about 100 sparkling necklaces, 14 layers of clothing in every clashing pattern possible, thick makeup and a pack of Fantasia cigarettes. My voice was hoarse and slow, like a ’40s-era lounge singer.
The video starts with us sitting on Mike’s stoop on Sixth Avenue and Garfield Place in Park Slope, talking with a group of moon-faced teenagers. I guess I already had the ‘‘marry Mike’’ campaign going because I got each of those kids to say, ‘‘You should marry Jaime.’’ In my hip-hop drawl, I started reciting lines from ‘‘Romeo and Juliet.’’ Then the kids chanted with me: ‘‘roses smelling sweet!’’ You can see they’re mesmerized and confused by this pseudo-adult, crazed, clad in a tutu. At the end of the exchange I said, ‘‘You babies are all right!’’ Then I jumped into some Eminem lyrics.
The next scene on the tape is me showing the camera different album covers and singing songs from each album. I’m wearing a cowboy hat, gold pants, a fluorescent flower skirt and all the necklaces in the world. I pause at ‘‘Sweeney Todd’’ and say, ‘‘Oh, this one’s about eating people, so, that’s cool.’’ Mike, off-camera, peppers me with questions, asking me to hold the albums higher or lower or to the side.
The next morning I set up the camera so the lens’s point of view shows what I’ve made — kumquat-and-avocado salad, cubed PowerBars and a glass of wine. I videotape Mike waking up. He negotiates for more sleeping time. I clearly hadn’t slept at all and was now wearing a silver-flecked red bra and a gold skirt. He finally acknowledges me by eating a PowerBar. I say Baruch atah Adonai over the cup of wine, borrowing from the Hebrew prayer. I whisper it as if my voice is a direct line to God. Mike asks me what I’m going to do today.
‘‘Today, I’m going to contact MTV to debate Gore, Bush or Tipper Gore. I hope it’s Tipper. I have a lot of work to do today.’’ Pause. ‘‘I have to change the world.’’
Mike asks me why I’m holding an avocado pit in my hand. ‘‘I saved the pit so we could plant it wherever we decide to land,’’ I say. Then I start talking about a singing toilet bowl, a scene from the musical I had written.
The last fragment of the tape captures that same day at dusk. The camera is pointed toward the floor, and I am dragging Mike up to the roof. You can hear the fatigue in his voice and the growing irritation. He’s resisting, while I’m guiding him upstairs. ‘‘Why are we going on the roof?’’ he asks.
We have to, I insist. He threatens to turn off the camcorder. I ask him to point it at me. Then, on bended knee, I ask him to marry me. ‘‘It’s all set up,’’ I say. The picture turns to snow.
After I watched the tape last year, I chatted with Mike, who is still a close friend. ‘‘I was always a little jealous of what you went through,’’ he told me. ‘‘You’ve had an experience that so few people have had. You’ve lost your mind entirely. It’s almost like you’ve been someone else.’’
What I saw was someone who resembled me, looked related to me, whom I remembered being. It was me without lithium.
After that episode, I went back on lithium and stayed on it, despite the health risks, which include increased thirst, weight gain and memory loss and, more rarely, thyroid deterioration, kidney dysfunction and the same dullness and lethargy experienced by Cade’s guinea pigs. I was scared by what happened when I went off it. Some people who take lithium feel robbed of their natural personality. But for me, at a certain point the mania takes over, and my actions become unbearable, to me and to others. Toward the end of my last episode, I was such a menace that my mother hired a minder to watch me, a Caribbean woman named Alma who would braid my hair into cornrows and take me to 99-cent stores.

I wanted a calmer life. So for the next 13 years, I took my three pink capsules and all was well. I wrote a book, I learned how to cook in an Italian-restaurant kitchen, I had a few relationships that lasted longer than a month, I wrote, I boxed, I traveled, I painted, I took my pills. I was fine.
Then, last fall, I saw my primary physician — and he sent me to the nearest emergency room. He was alarmed at my combination of high creatinine levels, damaged kidneys and heart-attack-level blood pressure (185/130). At Mount Sinai Hospital, my doctor’s fears were confirmed in a matter of days: My kidneys were irreparably damaged, an ‘‘uncommon but not rare’’ side effect of long-term lithium use. I was told I could phase out lithium and start another medication, or face dialysis and a kidney transplant in 10 years.
It doesn’t really feel like an obvious choice; it just feels like two bad options. Switching meds might mean the return of cornrowed, Eminem-obsessed Jamya and many seasonal gourds. Yet tubing up and cleansing my blood until I get a stranger’s kidney quilted into the rest of my insides is hardly more appealing. Test results indicate that my kidneys are working about half as well as they should; Maria DeVita, a nephrologist at Lenox Hill Hospital, told me that if I am to switch to preserve the kidney function I have left, ‘‘the time to strike is now.’’
When I start tapering off lithium a month or two from now, Schwartz will prescribe Depakote, a medicine used to treat bipolar disorder as well as seizures and migraines. The only way to know whether it works is if I don’t have a manic episode. And the idea of waiting for that terrifies me. My boyfriend of three and a half years doesn’t know what I’m like when I’m manic. There’s nothing that I can say that will prepare him. If it happens again, I’m worried I’ll run off and ride the rails or that I’ll be accidentally unfaithful or that I’ll insist on wearing metallic unitards and Mexican wrestling masks or that, worst of all, I just won’t be me, and he won’t be able to remember who I am or that I’m in there somewhere. I worry that without lithium I will lose my job, my partner, my home, my mind … because I’ve been through all this. I don’t believe in God, but I believe in lithium.
Before leaping into the worrisome unknown, I decided to travel to one of the grandest, most delusional places of all, the world’s largest reserve of lithium, in Bolivia. I would make a symbolic pilgrimage to the wellspring of my sanity.
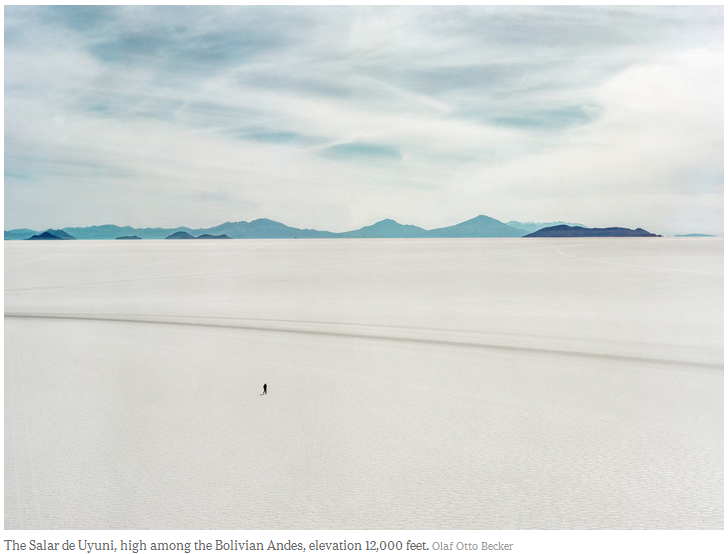
The vastness of Salar de Uyuni is intensified by its mind-bending, flesh-burning, breathtaking altitude. The salt flats spread out 12,000 feet above sea level and bring to mind the biggest, most perfect ice-skating pond imaginable. This part of southern Bolivia consists of 4,000 square miles of what were once prehistoric lakes, now dried up into crust and brine. Scientists say it took three minutes following the Big Bang, 13.7 billion years ago, for the first three elements to emerge — helium, hydrogen and then trace amounts of lithium, atomic number 3. Gazing out at the horizon here in Salar de Uyuni feels like looking back into those earliest moments of the universe. Nearby you can see natural hot springs and the Sol de Mañana, a geothermal spot pockmarked with steamy craters burping boiling mud. The place feels like a hallucination; there’s an island populated by century-old cactuses, a blood-red lagoon, flocks of hot pink wild flamingos and piles of a blindingly white crystalline substance.
There were tire tracks in the salt from four-by-fours. Off in the distance lay an isolated processing plant, christened in 2013 by the Bolivian president, Evo Morales. Evaporation ponds checkered the endless white expanse with shades of aqua.
I walked the crusted, jigsaw surface. I wanted to feel and taste its granularity and saltiness. The far-off Andean peaks floated dreamily, with no visible foundation. As I ran between the salt mounds, cracks accompanied each step. My hiking-boot footprints flooded with milky saltwater. I was so breathless, so thirsty, so thrilled. If ever there has been a perfect backdrop for a grandiose delusion, it is the Salar de Uyuni.
The lithium we have on Earth now — part stardust, part primordial dust and part earth dust — is a constituent part of our planet, one that sometimes shapes personalities. The thought occurred to me that maybe my taking lithium prophesied a lithium-dependent future, connecting it to a past when our world was birthed in fiery lithium explosions. Maybe that capsule filled with a salt, the one that allowed me to function, tethered past, present and future together. But then, extravagant prophecies built on the miraculous powers of a prehistoric element reek of mania.
After a few days of trekking, I stopped at a camp and slept in a building made of salt bricks — a lithium igloo. I sat in the nearby hot springs, in water naturally laden with high concentrations of lithium, and watched the steam rise on the moonshine horizon. If I soaked in this warm bath long enough, I thought, maybe it wouldn’t feel so bad to let go of my medicine.
Send a Message
Dr. Fieve’s Books